
Learning from Reports to Prevent Future Deaths in Mental Health settings - A Review of PFDs nationally 2022-2023
Whilst the main purpose of an inquest is to determine how a person came by their death, a coroner must also consider whether the evidence reveals ongoing concerning circumstances that create a risk of other deaths occurring in the future. Where such a risk exists, a coroner is under a duty to issue a report to Prevent Future Deaths, commonly known as a PFD report (or a Regulation 28 report).
In a healthcare context, a PFD report can be an important tool to improve public health, welfare and safety. Healthcare organisations can learn and improve not only from PFD reports that are issued directly to them, but also from PFD reports concerning organisations of a similar nature. With that in mind, we have reviewed 34 PFD reports concerning mental health related deaths, which were published between June 2022 and June 2023. We have analysed these reports to identify common themes and issues arising nationwide.
Summary
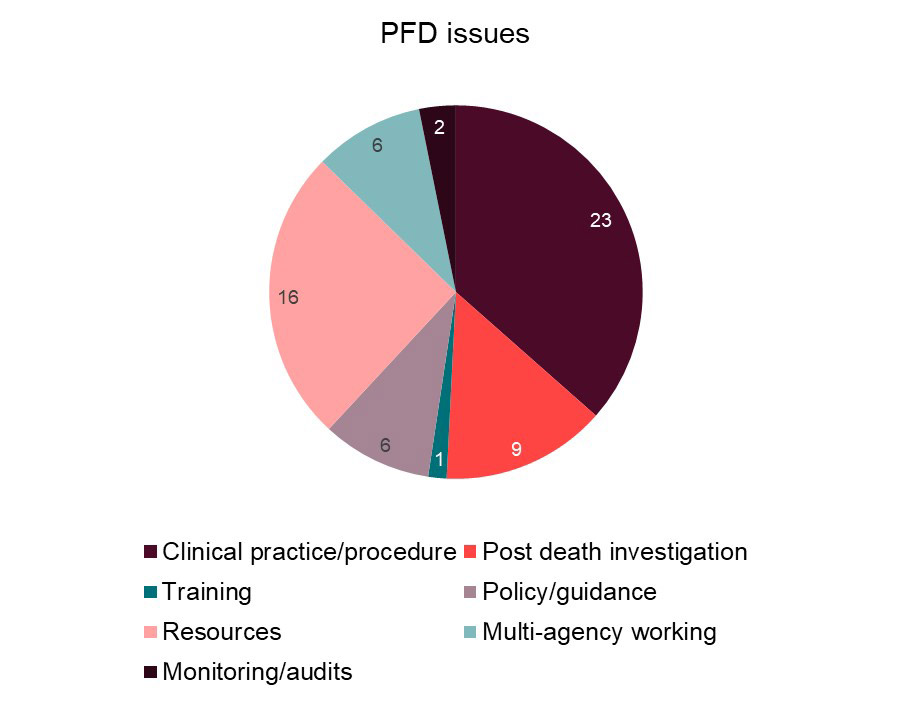
A PFD report can refer to multiple issues or risks that have arisen out of one inquest. We identified 63 key issues arising from the 34 PFD reports we looked at. We considered that those 63 issues could be broken down into seven main themes or categories – clinical practice/procedure, training, resources, monitoring/audits, post death investigation, policy/guidance and multi-agency working. The chart below summarises how frequently each issue arose:
Clinical practice or procedure
Issues relating to clinical practice and procedure were varied. However, a common issue that arose was in relation to risk assessments and risk management plans. Several coroners were concerned that risk assessments were not sufficiently detailed. Further, that risk management or care plans were not comprehensive enough to manage the identified risks, or in some instances not created at all. As one Senior Coroner noted, “There was a lack of a clear clinical assessment and plan to investigate and deal with repeated self-harm attempts that could result in serious injury or death as well as the repeated access to and use of ligatures.”
The failure to involve family members and carers in risk assessments and risk management plans was also identified in a number of inquests.
Insufficient patient observations were another common issue. In several cases, patient observations were not being completed as directed and accurate records were not being kept by staff.
Resources
“Resources” encompassed staff shortages, insufficient service provision, funding issues, long waiting times and inadequate assessment tools. It was highlighted in two inquests that there is a lack of mental health services for older adults. One inquest heard that older age psychiatric teams are poorly resourced nationally. Coroners raised concerns about the shortage of inpatient beds, insufficient psychotherapy community services and a lack of establishments suitably designed for dual physical and mental health needs in later life.
The underfunding of Child and Adolescent Mental Health Services (CAMHS) was also highlighted. One coroner raised concerns about long waiting times for children to be assessed and the shortage of child psychiatrists, psychologists and mental health nurses. One Senior Coroner commented that, “It became very clear during the inquest that there is significant under funding of the local mental health Trust who, like many mental health Trusts, have seen an explosion of referrals to their CAMHS service. Despite the increase in numbers accessing CAMHS there has not been any relative increase in resources to meet this demand and therefore the current position is unsustainable and it is putting many young people’s lives at risk.” Those concerns were addressed to the Secretary of State for Health and Social Care to respond to.
Two inquests also raised concerns about care coordinators in community mental health teams (CMHTs). It was highlighted that care coordinators typically have the most comprehensive view of a patient, however, CMHTs often do not have enough care coordinators. Coroners impressed the need for more funding to be made available to CMHTs, but also for Trusts to make the role more attractive and for there to be more consistency across Trusts as to how care coordinators are expected to fulfil their role. One Area Coroner noted that, “There are not enough care coordinators within the Trust and there are high turnovers of staff. Efforts need to be made to make the post of care coordinator more attractive. There has been an increase in the number of referrals coming into the service. There has been no commensurate increase in the number of care co-ordinators.”
One inquest focussed on a Trust’s Liaison and Diversion (L&D) service. The coroner highlighted that it was originally intended that L&D services would commission psychiatrists, but this did not ever come to fruition. After hearing expert evidence, the coroner concluded that L&D services need readily available advice and support from a consultant psychiatrist. The coroner’s concern was addressed to NHS England to answer.
One coroner raised concerns about the Wales Applied Risk Research Network (WARRN) assessment tool, which is used throughout Wales. The coroner considered that there were flaws with the format and layout of the WARRN, and that it did not provide a professional with clear and easily viewable information as to how a person’s risk of self-harm had fluctuated or changed. The coroner was concerned this could lead to an underestimation of risk and sub-optimal risk management measures being put in place.
Post death investigations
In nine inquests, coroners were either concerned that an inadequate post death investigation had been conducted by (or on behalf of) the healthcare body, or insufficient learning/remedial action had been implemented following the patient’s death. In one inquest, even when the healthcare organisation involved had commissioned an external company to conduct a review of the death, the coroner did not consider the investigation to be sufficient. The authors did not obtain all the relevant documents, did not ask staff to prepare statements and failed to investigate important matters. In another inquest, a Senior Coroner found that, “The Trust’s internal investigation did not consider the full extent of the deceased’s contacts with mental health services, lacked any meaningful critical analysis of events and omitted to seek to explore fundamental issues such as access to services from the patient’s perspective. As a consequence, the Trust has not taken the opportunity to learn from the death.”
Concerns were raised in several inquests that the family of the deceased had not been included in the post death investigation, even when the family had been involved in caring for the deceased prior to their death.
Policy or guidance
On a local level, one coroner raised concerns that the staff involved in a particular inquest gave conflicting and unclear evidence about Trust policies, namely referral processes into community teams and patient response times. Another coroner highlighted that a Trust did not have a specific policy regarding sexual harassment or assault, or a policy focusing specifically on communication with family members, and raised this as a concern.
On a national level, one coroner wrote to the Department of Health and Social Care (DHSC), highlighting the absence of national guidance for perimeter fencing and security outside areas of mental health locked wards. In another inquest, the DHSC was also asked to consider extending the section 136 Mental Health Act powers so that a person could be detained for a few days in order to help him through a period of crisis. (In its response to the PFD, the DHSC did not agree to do this.)
Multi-agency working
Concerns with multi-agency working were raised in six inquests. One coroner highlighted the complex relationship between epilepsy and mental health, and expressed concern about the “general lack of communication throughout the NHS between community psychiatric teams and neurology teams, across England and Wales.” Another coroner expressed concern about the inadequate information sharing between a patient’s GP and their mental health team.
Comment
Many of the themes we found were similar, so it will be helpful for mental health providers and commissioners to reflect on these when considering their own systems, processes and investigations. Trusts are now being asked to improve learning more generally under the Patient Safety Incident Response Framework (PSIRF). The PSIRF sets out the NHS’s approach to developing and maintaining effective systems and processes for responding to patient safety incidents for the purpose of learning and improving patient safety. Browne Jacobson has extensive experience of advising mental healthcare providers and commissioner on inquest processes and procedures, including PFD reports, investigations and representation at inquest.
If you would like further advice or guidance on inquests or any of the issues highlighted in this article, please do get in touch. From the outset of a matter, we provide support at whatever level your team needs, from standalone reviews of statements and internal investigations to full advice on legal issues, disclosure of documents and likely determinations. Many of our team have worked in house and therefore have detailed insight into what clients need and want from their legal support.
We support in-house teams through our popular ‘Shared Insights’ forum which brings together in-house teams from across the country, and shares knowledge on the biggest issues facing organisations. Our ‘Mock Inquest training sessions’ also provide valuable practical advice and tools for governance and risk, complaints, family liaison and in-house legal teams.

You may be interested in...

First decision on the Crime and Policing Act 2026: Scope of new limitation regime confined to sexual abuse claims

Shared Insights: Mental capacity, care and consent: Applying the legal framework in practice

Mock Court of Protection and Mental Capacity Act training course

Mindful insights: June 2026

Spotlight on: Anya Yaseen, Senior Associate

Re XY: What healthcare providers need to know about welfare deputies' powers

Supreme Court overrules Cheshire West: Deprivation of liberty law reshaped for health and social care settings

LM v Sussex ICB: Can you have capacity for residence if you lack capacity for care?

Mock inquest training course

Shared Insights: Impact of the Patient Safety Incident Response Framework (PSIRF) on preparing for inquests

The impact of the Patient Safety Incident Response Framework (PSIRF) on preparing for inquests: Navigating the evidential gap

Patient Safety Incident Response Framework (PSIRF) inquest toolkit

Mental health crisis care and the legal gap in emergency departments

Self-referral to regulatory bodies following an inquest

Shared Insights: Coroner's question time

No "clinical decision" exemption from best interests

MNSI data shows a fall in reported cases of HIE in England

Independent Investigation into Maternity and Neonatal Services Interim Report: Proactive steps for NHS Trusts

Independent Investigation into Maternity and Neonatal Services Interim Report: Key findings and next steps

Mindful insights: February 2026

Mental Health Act 2025 new provisions come into effect: Legal comment

Browne Jacobson barrister and solicitor appointed as Deputy District Judges

Newsletter guidance for healthcare providers on PSIRF and inquests

The Mental Health Act 2025: Provisions coming into force in February 2026

Behind bars: The hidden health crisis in England's prisons

Supreme Court ruling: Illegality defence applies despite insanity acquittal
Mental Health Bill receives royal assent
Mental Health Act 2025: Legal comment as Bill receives royal assent

Injunctions in the Court of Protection: Protecting vulnerable adults from obstructive behaviour

Shared insights: Managing children with complex needs in crisis

Shared insights: Corporate and gross negligence manslaughter in the health and care sector

Liberty Protection Safeguards: 2026 consultation announced and Northern Ireland Cheshire West challenge

Self-neglect and capacity: Insights from recent regulatory and safeguarding adult reviews

The Public Office (Accountability) Bill: A new era for inquests, inquiries and public accountability

Mindful insights: October 2025

Shared Insights: Coroner's question time

Chief Coroner’s guidance on trans individuals: What health and social care providers need to know

Spotlight on: Laura Thomas, Associate

Court of Protection lifts treatment restrictions for young woman with severe anorexia nervosa
